Jun 09 2016
Reimagining the Aanganwadi Programme

We dream of a strong and progressive India. A nation is the sum total of its people and therefore it is important to ensure that India becomes inclusive and ensures that each citizen has access to nutrition, health and opportunity to chase their dreams. In the year 1975, Government of India established “Integrated Child Development Services”, popularly known as ICDS. The ICDS programme revolves around the Anganwadi centres situated in villages across India. One of the main objectives of the ICDS programme is to improve health of a child by providing nutritional food supplies. The scheme extends access to nutritional food to expectant mothers and then the new born to help reduce infant mortality rate and other malnutrition related problems. The Anganwadi system, more than 1.3 Million strong, is the vital link in meeting the objectives of the ICDS programme. Literal meaning of the Hindi word “anganwadi” is “courtyard”. Today a typical Anganwadi provides basic health services and is the fulcrum of the public health-care system in rural India. One can observe following activities at a typical Anganwadi-
-
Basic healthcare counselling to women including contraceptive counselling
-
Nutrition education, including supply of nutritional supplements– such as hot food served in the Anganwadi and Take Home Rations (THR), immunisation, health check-up and referral services in coordination with public health systems
-
A day-care activity centre, or a preschool, for 3 to 6 year old children
How does the Anganwadi Function?
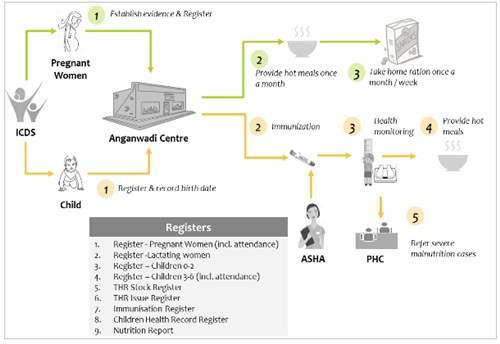
Two types of beneficiaries visit Anganwadi centres- Pregnant Women/Lactating Mothers and Children. The programme provides Take Home Rations (THR) consisting of dry, easy to prepare and eat food products/nutritional supplements for the benefit of the women (pregnant and lactating mothers) and the children aged 0-2years who stayed at home with their mothers. There are nine types of registers/reports which are maintained at Anganwadi (enlisted in pictorial depiction). Complete information regarding beneficiaries is recorded in these registers, which includes attendance, registration details, immunization details and most importantly health records. Using these registers, one can identify a mother or child who is malnourished and, initiate a preventive action plan.
The challenges faced in the current process
Data entry and monitoring: The presence of huge number of registers and records make data entry, monitoring and analysis very difficult. Moreover, the availability of the data at a central location is either not possible or delayed. The task of aggregating the data at district, state or country level becomes very slow, complex and error prone.
Beneficiary identification: The problem of identifying a beneficiary and avoiding ghost beneficiaries is an age-old problem and a big nemesis of any large government-run projects. The current system does not ensure that the benefits are received by the intended beneficiaries only.
Transfer/Relocation of beneficiary: Generally, Anganwadi caters to a local people of the village and Anganwadi workers know beneficiary personally. But, when a beneficiary is relocated from one place to another it becomes very difficult for her to receive benefits due to sheer disconnect between two Anganwadi centres.
What can be done to make this important programme meet its goals?
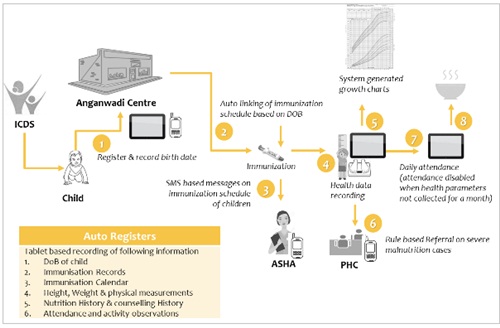
Using technology to capture the beneficiary data, attendance, immunization and health information electronically through a mobile or a tablet could be the solution. This would enable meaningful monitoring. For example, a system could be established to send reminders to the beneficiaries, when they are absent or miss visiting the designated Anganwadi for a period of time. Such a system would also enable the authentication of the beneficiary using AADHAR or mobile based validation process to systematically identify the beneficiary.
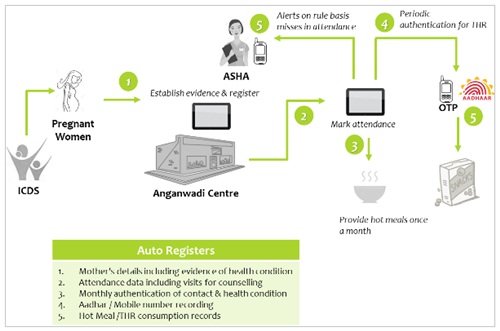
Paperless data management: Day-to-day data capture, monitoring and analysis of daily activity in paperless form empowers the programme managers to understand exceptions and resolve issues related to services, beneficiary experience, especially delay and errors in benefit delivery. Once the beneficiary data is available on a server or cloud, seamless monitoring and proactive action with specific reference to a whole region or an individual, becomes simple. Once the data is available in digital format, various rule based triggers can also be generated, for example reminders to absent beneficiaries, reminders about vaccination orother customized counselling or beneficiary education).
AADHAR/Mobile based verification: By enabling AADHAR/Mobile based verification, the issue of ghost beneficiaries can be addressed. Identification of the beneficiary is core to the success of benefit delivery. Established verification process will pave way for dynamic beneficiary management, such as relocation or transfer of beneficiary, temporary change in status, specialised one-on-one benefits for specific conditions and so on. Once this is established a beneficiary need not be tied to a location or a specific Anganwadi unit. By simply producing an AADHAR card or Mobile based verification the beneficiaries’ entitlement would be validated and services could be universally accessed from any Anganwadi with access to the system.
Timely and seamless information flow are often the ingredients that make governance effective. This programme is addressing the utmost important segment, delivering access to nutrition. If this programme succeeds and meets its objectives, we can guarantee the emergence of a healthy and strong India of our dreams. Let’s re-imagine and realise our potential!
Recent Posts